Bendamustine – Targeted Therapy
Known as original brand(s)
Treanda, Ribomustin
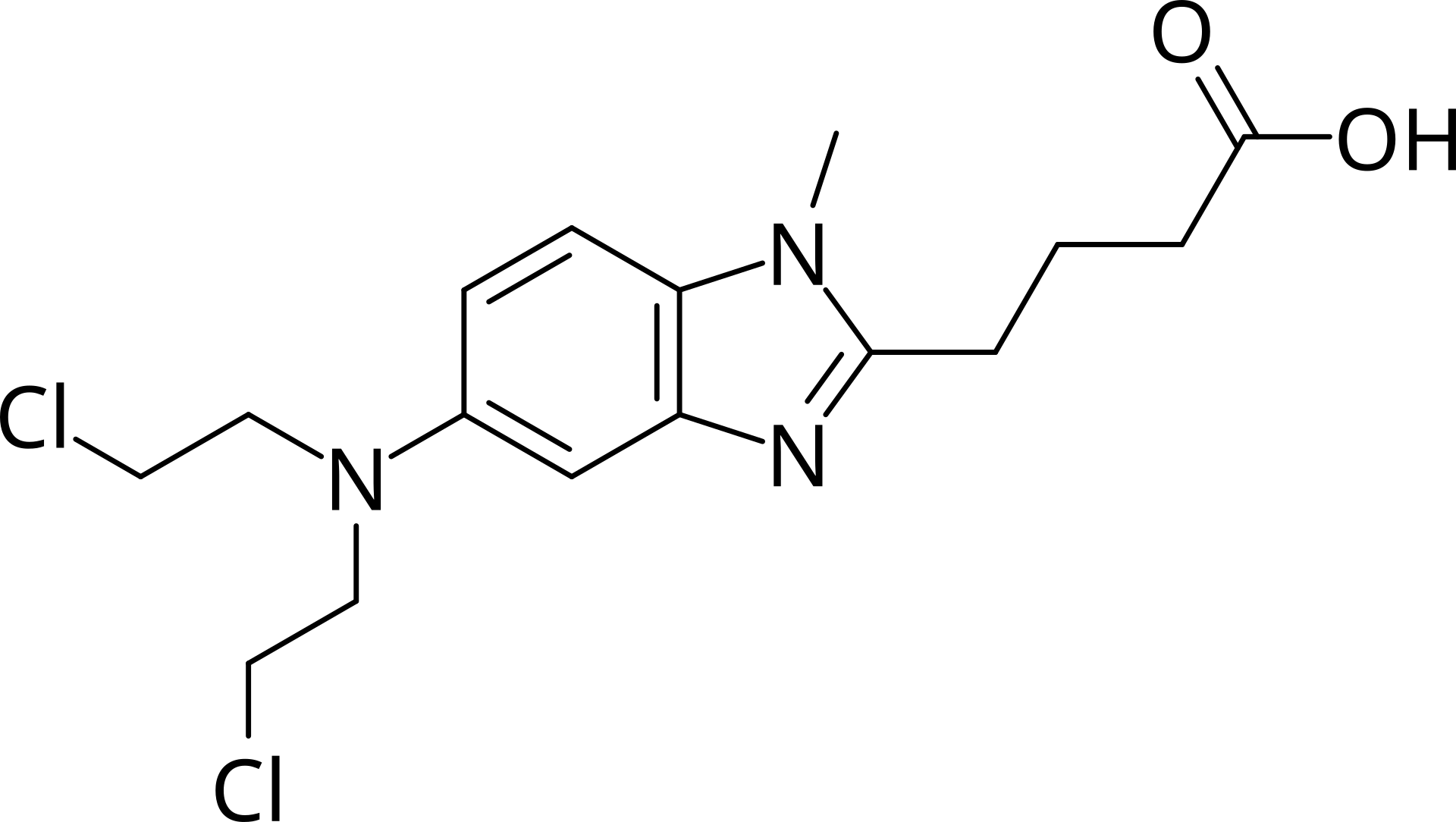
Bendamustine is a unique antitumor agent that combines the properties of alkylating compounds and antimetabolites (purine analogs). The drug is intended for systemic chemotherapy of various types of malignant neoplasms of lymphoid and hematopoietic tissues.
The mechanism of action of bendamustine is based on the formation of strong cross-links between the DNA strands of cancer cells. This causes multiple breaks in the genetic material, making further cell division and repair impossible. Due to its hybrid structure, bendamustine remains active even in cases where the tumor shows resistance to classic alkylating agents (e.g., cyclophosphamide). The drug induces programmed cell death (apoptosis) and effectively targets slowly dividing cells.
Bendamustine is administered by intravenous infusion and is often used in combination with monoclonal antibodies or other chemotherapeutic agents, demonstrating high efficacy with a low level of nervous system side effects.
Indications
Bendamustine is used in hematology and oncology for the treatment of the following conditions:
- Chronic Lymphocytic Leukemia (CLL): first-line therapy for patients for whom fludarabine combination therapy is not appropriate.
- Indolent Non-Hodgkin Lymphomas: used as monotherapy in patients who have progressed during or following treatment with rituximab.
- Multiple Myeloma: used in combination with prednisone for patients older than 65 who are not candidates for stem cell transplantation.
- Mantle Cell Lymphoma: as part of combination regimens to achieve long-term remission.
Dosage and administration
The bendamustine dosing regimen is established individually based on body surface area and the type of disease.
- Standard Dose: typically ranges from 70 mg/m² to 120 mg/m² of the patient's body surface area.
- Administration Method: the drug is administered as an intravenous infusion over 30–60 minutes.
- Cycling: therapy is administered in cycles (e.g., on Days 1 and 2 of a 28-day cycle). The number of cycles is determined by the treating physician.
- Preparation: before administration, the powder must be fully dissolved and diluted in saline to the required concentration.
- Dose Adjustment: if hematologic toxicity develops (decrease in white blood cells or platelets), the next cycle may be delayed or the dose reduced.
