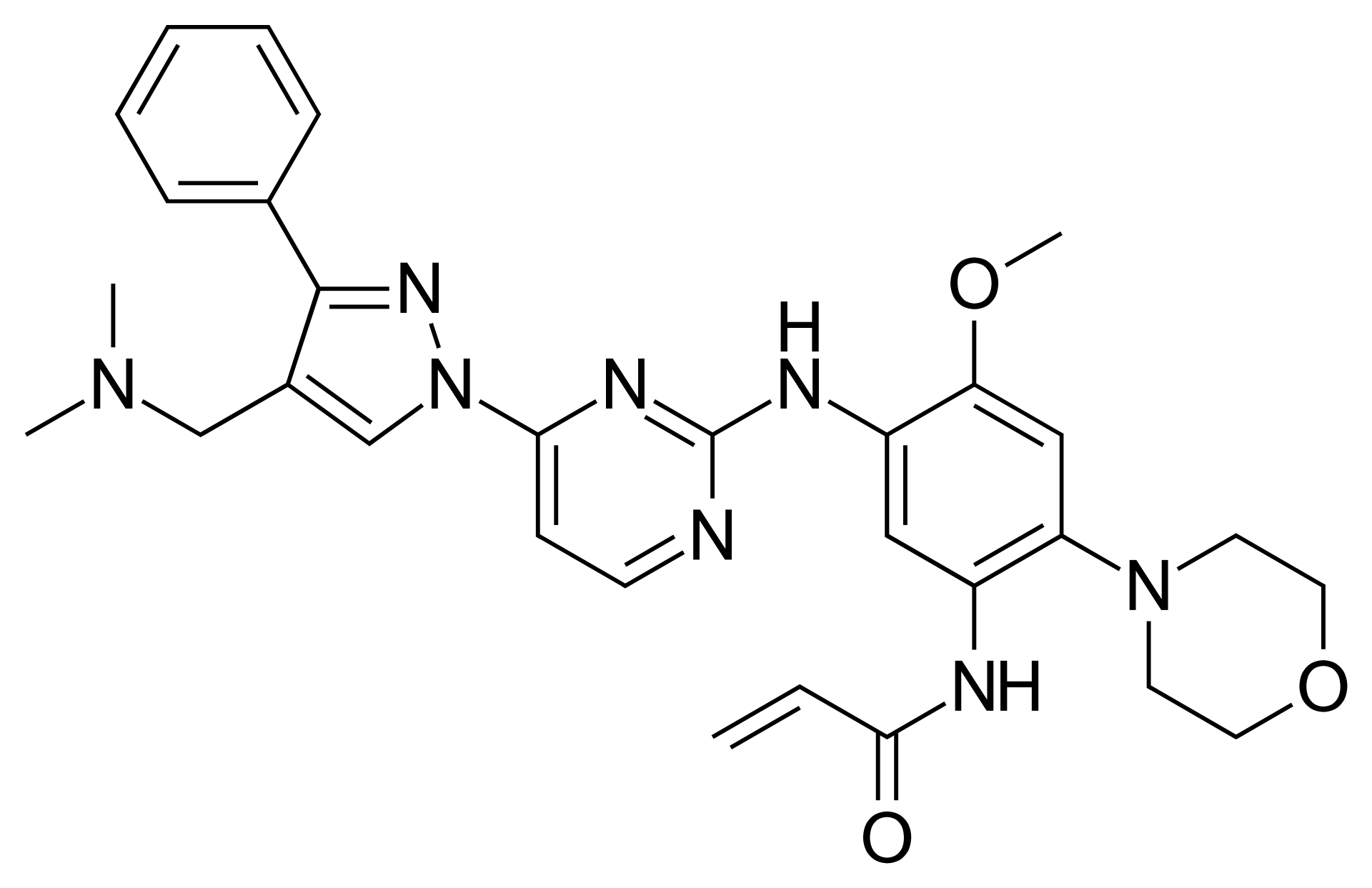
Lazertinib – Third-Generation EGFR Tyrosine Kinase Inhibitor
Known as original brand(s)
Leclaza
Lazertinib is an oral, irreversible, highly selective, third-generation small-molecule epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor engineered for the systemic targeted therapy of non-small cell lung cancer. The mechanism of action of lazertinib involves covalent binding to the kinase domain of mutant forms of the EGFR receptor, including activating mutations (exon 19 deletions and exon 21 L858R substitution), as well as the secondary T790M resistance mutation. The drug selectively blocks receptor autophosphorylation, resulting in the complete disruption of downstream oncogenic signaling cascades through the MAPK/ERK and PI3K/AKT/mTOR pathways, thereby inducing pronounced apoptosis and cell cycle arrest in tumor cells. A key pharmacological feature of lazertinib is its minimal affinity for wild-type (native) EGFR, which significantly reduces systemic toxicities affecting cutaneous tissues and the gastrointestinal tract.
The clinical uniqueness of lazertinib lies in its high systemic exposure and its excellent ability to penetrate the blood-brain barrier, enabling deep and durable intracranial responses in patients with metastatic central nervous system lesions. The drug exhibits good oral bioavailability, which is not critically altered by food intake. Peak plasma exposure is achieved within a median of 3 to 4 hours post-dose. Lazertinib distributes extensively into tissues and is primarily metabolized in the liver via the cytochrome P450 system, predominantly by the CYP3A4 isoenzyme. The elimination half-life of the active compound ranges from approximately 24 to 36 hours, ensuring stable therapeutic concentrations. Systemic clearance occurs predominantly through the intestines in the feces, with a minor fraction cleared via the kidneys in the urine.
The drug is administered orally. Initiating therapy requires mandatory prior molecular-genetic confirmation of the corresponding EGFR mutations in tumor tissue samples or circulating tumor DNA. Ongoing treatment necessitates regular electrocardiogram monitoring and assessment of left ventricular cardiac function.
Indications
Lazertinib is indicated as a systemic targeted monotherapy or combination treatment for adult patients presenting with the following malignant neoplasm:
- Non-Small Cell Lung Cancer (NSCLC): first-line treatment of adult patients with locally advanced or metastatic non-small cell lung cancer harboring activating EGFR mutations (exon 19 deletion or exon 21 L858R substitution), as well as the treatment of patients with disease progression on or after prior EGFR tyrosine kinase inhibitor therapy of the first or second generation in the presence of the confirmed T790M resistance mutation.
Dosage and administration
The dosing regimen of lazertinib is established individually, based on clinical trial data, and strictly mandates continuous daily administration.
- Standard Therapeutic Dose: the recommended starting dose is 240 mg taken orally once daily. The drug must be taken daily, at approximately the same time each day.
- Combination Treatment Schedule: when utilized as part of a combination precision therapy, lazertinib is administered at the standard dose of 240 mg once daily continuously, alongside the concurrent administration of companion monoclonal antibodies or chemotherapeutic agents according to their specific protocols.
- Administration Method: tablets are taken orally, with or without food, and must be swallowed whole with a sufficient amount of water. Tablets must not be broken, crushed, dissolved, or chewed during handling.
- Missed Dose: if a scheduled dose is delayed by less than 12 hours, the patient must take the missed dose immediately. If the delay exceeds 12 hours, that dose must be skipped entirely, and the patient should take the next dose at the regular scheduled time. Taking a double dose is strictly prohibited. If vomiting occurs after taking a tablet, an additional dose should not be administered.
- Dose Modification for Toxicity: if severe adverse reactions develop (such as interstitial lung disease, prominent QTc interval prolongation, or severe cutaneous toxicity), therapy must be temporarily withheld. Upon clinical resolution of symptoms, treatment is resumed with step-down dose reductions: first to 160 mg once daily, then to 80 mg once daily. If a patient cannot tolerate 80 mg once daily, the drug must be permanently discontinued.
