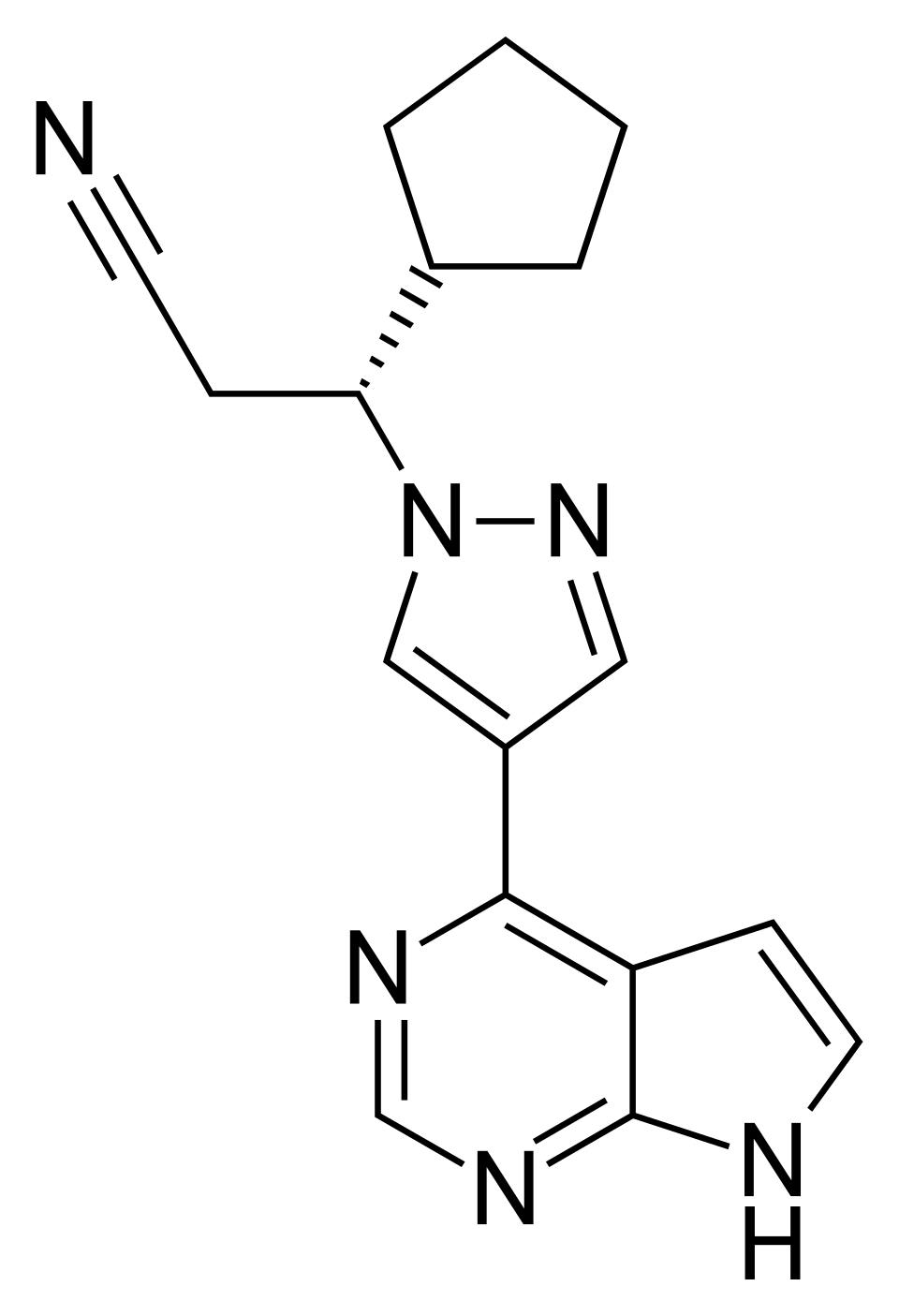
Ruxolitinib – Selective JAK1 and JAK2 Inhibitor Targeted Therapy
Known as original brand(s)
Jakafi, Jakavi
Ruxolitinib is an oral, potent, and selective inhibitor of the Janus associated kinases (JAK) type JAK1 and JAK2. The drug was developed for the pathogenic targeted therapy of myeloproliferative neoplasms, including myelofibrosis and polycythemia vera, as well as for the management of severe graft-versus-host disease (GVHD). The mechanism of action of ruxolitinib is based on competitive inhibition of the ATP-binding domain of JAK1 and JAK2 kinases, which are pivotal mediators in the JAK-STAT signaling pathway. Disruption of this cascade prevents the phosphorylation and nuclear translocation of STAT proteins, resulting in powerful suppression of aberrant myeloid cell proliferation, reduction of pathological extramedullary hematopoiesis in the spleen, and a significant decrease in plasma concentrations of pro-inflammatory cytokines.
A unique clinical feature of ruxolitinib is its capacity to effectively control disease manifestations regardless of the presence or absence of the specific JAK2 V617F mutation. The drug fundamentally altered the therapeutic paradigm for patients with myelofibrosis, providing a pronounced and sustained reduction in spleen size (splenomegaly) and ameliorating debilitating constitutional symptoms such as night sweats, pruritus, fever, and weight loss. Ruxolitinib is rapidly and almost completely absorbed in the gastrointestinal tract following oral administration, exhibits a high degree of binding to plasma albumin, and is metabolized primarily in the liver via the cytochrome CYP3A4 isoenzyme. The elimination half-life is approximately 3 hours, requiring a twice-daily dosing regimen to maintain therapeutic efficacy.
The drug is administered orally. Therapy necessitates mandatory regular complete blood count monitoring to evaluate the degree of bone marrow suppression, particularly during the initial weeks of treatment.
Indications
Ruxolitinib is indicated for the treatment of adult and, in specific cases, pediatric patients with the following clinical conditions:
- Myelofibrosis: therapy for splenomegaly and/or constitutional symptoms in adult patients with intermediate or high-risk primary myelofibrosis, post-polycythemia vera myelofibrosis, or post-essential thrombocythemia myelofibrosis.
- Polycythemia Vera: treatment of adult patients with polycythemia vera who are resistant to or intolerant of hydroxyurea (hydroxycarbamide) therapy.
- Graft-Versus-Host Disease (GVHD): treatment of acute or chronic GVHD in patients aged 12 years and older who have an inadequate response to corticosteroids or other systemic therapies.
Dosage and administration
The dosing regimen of ruxolitinib is adjusted strictly individually based on baseline platelet count, the clinical indication, and patient tolerability.
- In Myelofibrosis (Starting Dose): the recommended dose is 20 mg orally twice daily for a platelet count greater than 200,000/μL; 15 mg twice daily for a count between 100,000 and 200,000/μL; and 5 mg twice daily for a count between 50,000 and 100,000/μL.
- In Polycythemia Vera: the recommended starting dose is 10 mg taken orally twice daily.
- In Graft-Versus-Host Disease (GVHD): the standard dose is 5 mg or 10 mg orally twice daily, depending on the baseline severity and clinical response.
- Administration Method: tablets are taken orally twice daily, at approximately the same times each day, with or without food, swallowed with a glass of water. Chewing the tablets is not recommended.
- Dose Adjustment for Cytopenia: if during the course of treatment the platelet count drops below 50,000/μL or the absolute neutrophil count falls below 500/μL, therapy should be withheld until counts recover.
- Special Warnings (CYP3A4): in patients concomitantly taking strong CYP3A4 inhibitors (e.g., ketoconazole, clarithromycin), the individual dose of ruxolitinib should be reduced by approximately 50%.


