Bicalutamide – Non-Steroidal Antiandrogen Therapy for Prostate Cancer
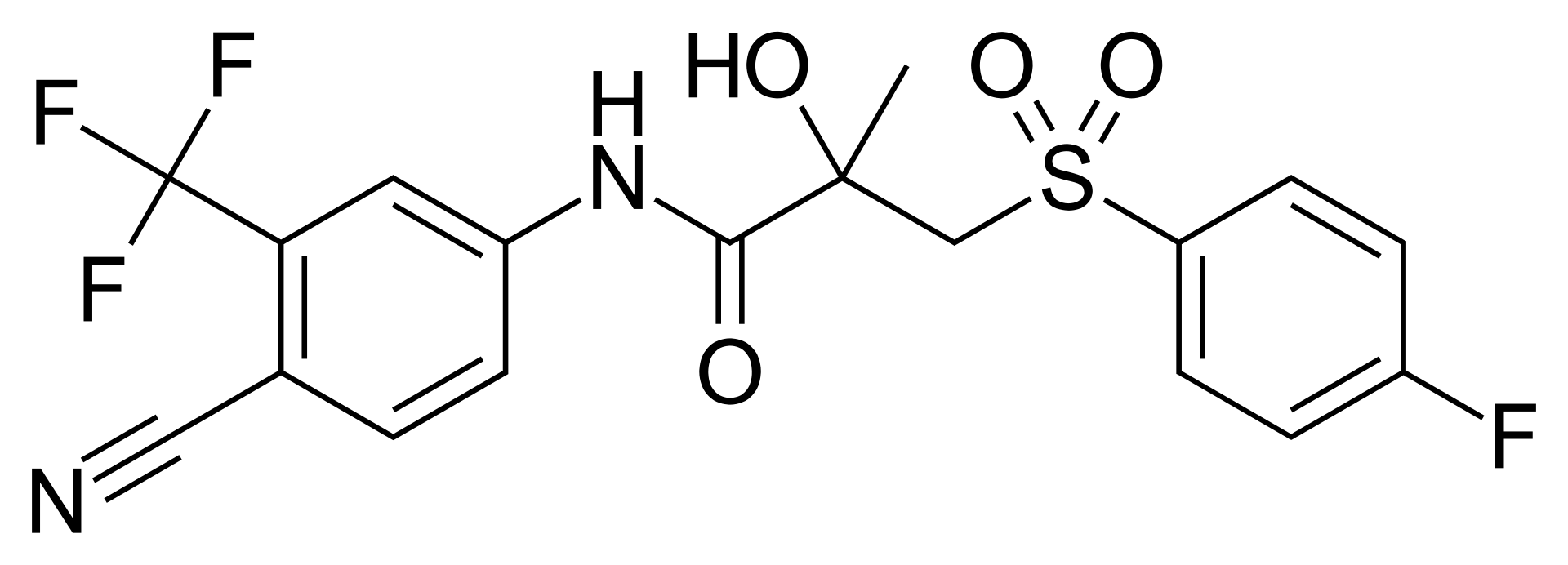
Bicalutamide is an oral, non-steroidal antiandrogen of first choice belonging to the phenoxybenzamide derivatives, engineered for the highly selective hormonal therapy of advanced prostate cancer. The mechanism of action of bicalutamide involves competitive binding to androgen receptors (AR) on the surface and within malignant cells. By occupying the binding domain, the drug effectively blocks receptor stimulation by endogenous androgens—namely testosterone and dihydrotestosterone (DHT). This halts the translocation of the receptor complex into the cell nucleus, suppresses the transcription of androgen-dependent target genes, and completely compromises mitotic signaling pathways. Consequently, this induces widespread apoptosis and involution of hormone-sensitive malignant prostate clones. Bicalutamide is a pure antiandrogen and, unlike steroidal alternatives, lacks any inherent internal hormonal (progestational, estrogenic, or glucocorticoid) activity.
The clinical uniqueness of bicalutamide lies in its ability to deliver a profound and sustained peripheral receptor blockade while maintaining a stable therapeutic plateau, making it suitable for both monotherapy and within maximal androgen blockade (MAB) combined with surgical castration or gonadotropin-releasing hormone (GnRH) analogues. The drug undergoes slow but complete absorption within the gastrointestinal tract following oral administration. Downstream pharmacodynamics are determined by optical isomerism: antiandrogen activity resides almost exclusively in the (R)-enantiomer, which features a prolonged elimination half-life from plasma (approximately 7 days). The drug is extensively metabolized in the liver via oxidation and subsequent glucuronidation mediated by cytochrome P450 isoenzymes. Metabolites are excreted in roughly equal proportions via the kidneys in the urine and through the intestines in the feces.
The drug is administered orally. Initiating therapy requires prior histological verification of prostate adenocarcinoma and baseline assessment of prostate-specific antigen (PSA) levels. Continuous laboratory monitoring of hepatic function parameters is mandatory throughout long-term treatment due to risks of delayed hepatotoxicity.
Indications
Bicalutamide is indicated as a systemic hormonal therapy for adult patients with the following malignant oncological condition:
- Advanced Prostate Cancer: treatment of locally advanced prostate cancer (as monotherapy or adjuvant therapy following radical prostatectomy or radiotherapy) or metastatic prostate cancer as part of combined maximal androgen blockade in conjunction with GnRH analogue therapy or surgical castration.
Dosage and administration
The dosing regimen of bicalutamide is continuous and structured for long-term daily administration, depending directly on the clinical stage of the disease and the selected therapeutic protocol.
- Standard Dose in Combination Therapy: the recommended dose for metastatic cancer within MAB (co-administered with a GnRH analogue) is 50 mg (one tablet) taken orally once daily. Treatment should be initiated concurrently with the GnRH analogue regimen.
- Standard Dose in Monotherapy: the recommended therapeutic dose for the management of locally advanced prostate cancer without metastases is 150 mg (three 50 mg tablets or one specialized 150 mg tablet) taken orally once daily.
- Schedule and Duration: the drug is taken daily without planned treatment breaks. Therapy must be maintained long-term (for months or years) as long as an objective clinical response (monitored by PSA levels) is sustained or until clear disease progression occurs.
- Administration Method: tablets must be swallowed whole at approximately the same time each day, with or without food. Tablets must not be broken or chewed, and should be administered with a sufficient volume of water.
- Missed Dose: if a scheduled dose is missed, an additional tablet should not be taken later that day, nor should the dose be doubled the following day. The patient must simply resume treatment with the next planned dose according to their regular schedule.
