Cholestyramine Resin – Bile Acid Sequestrant and Antihyperlipidemic Agent
Known as original brand(s)
Questran
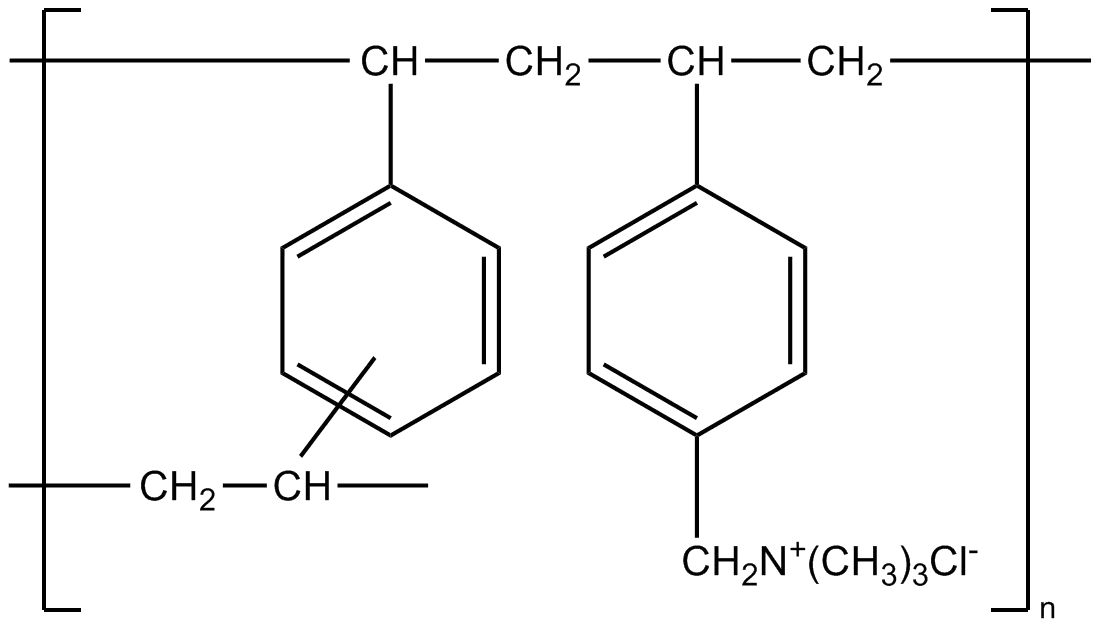
Cholestyramine Resin is an oral, lipid-lowering, and antihypercholesterolemic therapeutic agent formulated as a strongly basic anion-exchange resin (a copolymer of styrene and divinylbenzene containing quaternary ammonium groups in the chloride form). The mechanism of action of cholestyramine is purely physicochemical and transpires exclusively within the intestinal lumen without any systemic absorption of the resin into the bloodstream. Upon oral ingestion, cholestyramine molecules strongly bind (sequester) endogenous bile acids within the lumen of the small intestine via an anion-exchange process. The resulting insoluble complexes are fully excreted from the body in the feces. Interrupting the natural enterohepatic circulation of bile acids induces a sharp decline in their return to the liver. In response, hepatocytes upregulate the de novo synthesis of bile acids from cellular cholesterol via a feedback loop mechanism. This stimulates a significant increase in the expression of low-density lipoprotein (LDL) receptors on hepatic membranes, accelerating the clearance and systemic removal of atherogenic cholesterol from the circulation.
The clinical uniqueness of cholestyramine lies in its therapeutic versatility, extending far beyond the management of lipid panels. In addition to effectively reducing total cholesterol and LDL cholesterol levels, the drug is an indispensable tool for the pathologic management of severe pruritus associated with partial biliary obstruction or cholestatic liver diseases, effectively removing excess circulating bile acids deposited in the dermis. Cholestyramine is also widely utilized for the symptomatic relief of cholegenic diarrhea, which develops due to an excessive influx of bile acids into the colon (e.g., following ileal resection or cholecystectomy). The resin is completely insoluble in water and remains unaffected by gastrointestinal digestive enzymes. It is not absorbed and is eliminated unchanged in the fecal mass alongside the bound metabolites. Elimination half-life and systemic metabolism are absent due to the complete lack of systemic absorption.
The drug is administered orally as a pre-constituted suspension. Initiating therapy mandates regular laboratory monitoring of lipid profiles, prothrombin time tracking, and plasma folate concentrations (especially during long-term high-dose regimens). Because the resin can non-specifically bind co-administered medications, any other oral pharmaceuticals must be taken at least 1 hour before or 4 to 6 hours after cholestyramine administration.
Indications
Cholestyramine is indicated for the systemic symptomatic and pathologic therapy of adult and pediatric patients presenting with the following disorders and diseases:
- Hypercholesterolemia: reduction of elevated total cholesterol and low-density lipoprotein (LDL) cholesterol levels in patients with primary hypercholesterolemia (Fredrickson Type IIa) when dietary modifications alone prove inadequate.
- Cholestatic Pruritus: pathologic management and palliation of severe pruritus associated with partial biliary obstruction, primary biliary cholangitis, or other cholestatic syndromes.
- Cholegenic Diarrhea: symptomatic management of diarrhea induced by malabsorption and excessive accumulation of bile acids inside the intestinal lumen (following ileal resection, cholecystectomy, or associated with Crohn's disease).
Dosage and administration
The dosing regimen of cholestyramine must be individualized, with gradual dose titration employed to minimize gastrointestinal adverse effects.
- Standard Adult Dose: the initial dose is 4 g (one sachet or one level scoopful) taken orally 1–2 times daily. If clinically required, the dose is gradually escalated at weekly intervals to a maintenance dose of 8–24 g per day, divided into 2–6 administrations. The maximum daily dose is 36 g.
- Pediatric Regimen: the recommended therapeutic dose for pediatric patients over 6 years of age is calculated individually, typically starting at 240 mg per kilogram of body weight per day, split into 2–3 administrations. The total dose must not exceed standard adult limits.
- Administration Method: the dry powder must never be swallowed in its raw form due to the severe risk of aspiration. Prior to ingestion, each dose must be thoroughly mixed into 60–150 mL of liquid (water, fruit juice, non-carbonated beverages, soup, or pureed fruits) until a uniform suspension is obtained, and consumed immediately.
- Missed Dose: if a scheduled dose is missed, the patient should take it as soon as remembered, provided the interval to the next dose is long. If the next dose is near, the missed dose must be omitted entirely. Taking a double dose to compensate for a missed one is strictly prohibited.
- Co-administered Therapy Adjustments: all concurrent oral medications must be administered at least 1 hour before or 4 to 6 hours after the cholestyramine dose to avoid significant impairment of their gastrointestinal absorption.
