Ursodeoxycholic Acid – Hydrophilic Bile Acid Hepatoprotective Agent
Known as original brand(s)
Ursofalk, Ursosan
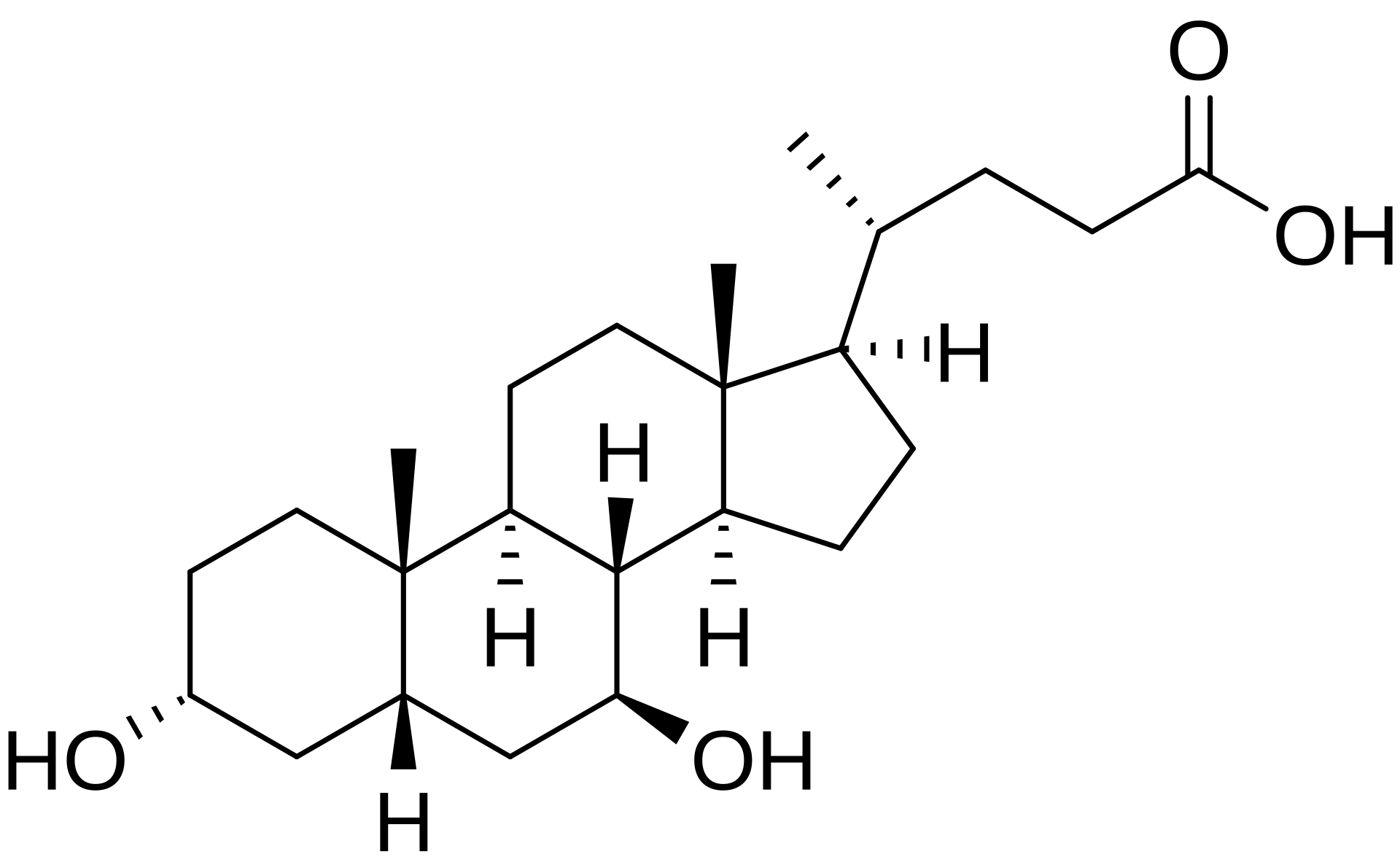
Ursodeoxycholic Acid (UDCA) is a hydrophilic, non-toxic tertiary bile acid that exists as a natural minor component of human bile and is utilized as a systemic hepatoprotective, cholelitholytic, and anticholestatic therapeutic agent. The mechanism of action of ursodeoxycholic acid is multifactorial. Upon oral administration, UDCA competitively displaces toxic, hydrophobic endogenous bile acids (such as chenodeoxycholic, deoxycholic, and lithocholic acids) from the circulating bile acid pool within the intestines and liver, significantly reducing their enterohepatic circulation. By shielding the membranes of hepatocytes and cholangiocytes from the cytolytic actions of these toxic acids, UDCA inserts directly into the phospholipid bilayer of cellular membranes, stabilizing their structure and enhancing resistance against damaging agents. Its cholelitholytic efficacy is driven by a reduction in hepatic cholesterol synthesis, decreased intestinal cholesterol absorption, and a subsequent lowering of the lithogenic index of bile. This facilitates the progressive dissolution of cholesterol-based gallstones and prevents the formation of new calculi.
The clinical uniqueness of ursodeoxycholic acid lies in its established ability to delay the progression of fibrosis and histological deterioration in patients presenting with primary biliary cholangitis (PBC), markedly improving hepatic biochemical panels and prolonging transplant-free survival. The drug exerts potent immunomodulatory effects: it represses the pathological overexpression of HLA class I molecules on hepatocytes and HLA class II molecules on cholangiocytes, mitigating autoimmune targeting, and dampens cell apoptosis triggered by toxic bile acid exposure. Following oral intake, UDCA is rapidly and passively absorbed in the jejunum and ileum (approximately 60–80%). During its initial hepatic pass, up to 70% of the drug is extracted by hepatocytes and conjugated with glycine and taurine. With continuous dosing, UDCA becomes the predominant bile acid in the blood plasma, accounting for up to 30–50% of the total circulating pool. It undergoes bacterial biotransformation in the gut into lithocholic acid, which is largely excreted in the feces, while a small portion is absorbed, sulfated by the liver, and subsequently eliminated. The elimination half-life ranges from approximately 3.5 to 5.8 days. Systemic clearance occurs predominantly through the intestines in the feces.
The drug is administered orally. Initiating therapy for gallstone dissolution strictly requires prior confirmation of the cholesterol nature of the stones, their radiolucent characteristics, and the preservation of normal gallbladder function. Ongoing treatment requires regular liver function monitoring (ALT, AST, GGT, and bilirubin levels) alongside ultrasonographic or radiological assessments of the biliary tract executed every 6 months.
Indications
Ursodeoxycholic acid is indicated for the systemic therapy of adult and pediatric patients presenting with the following hepatobiliary pathologies:
- Primary Biliary Cholangitis (PBC): pathologic management of primary biliary cholangitis (formerly designated as primary biliary cirrhosis) in patients without decompensated disease.
- Dissolution of Gallstones: dissolution of small-to-medium radiolucent cholesterol gallstones (measuring less than 15 mm in diameter) in patients possessing a functioning gallbladder, where surgical intervention is inappropriate or unfeasible.
- Biliary Reflux Gastritis: symptomatic management of gastritis induced by duodenogastric bile reflux.
- Mucoviscidosis (Cystic Fibrosis): treatment of hepatobiliary disorders associated with cystic fibrosis in pediatric patients aged 6 to 18 years.
- Other Cholestatic Conditions: comprehensive management of non-alcoholic steatohepatitis (NASH), chronic hepatitis of diverse etiologies featuring cholestatic syndrome, and primary sclerosing cholangitis (PSC).
Dosage and administration
The dosing regimen of ursodeoxycholic acid is customized based on individual body weight, the specific clinical indication, and mandates long-term, uninterrupted administration.
- Dose in Primary Biliary Cholangitis: the recommended daily dose is 10–15 mg per kilogram of body weight. During the initial 3 months of treatment, the daily dose should be divided into 2–3 administrations; following the stabilization of hepatic biochemical panels, the total dose may be taken once daily in the evening.
- Dose for Gallstone Dissolution: the recommended daily dose is 10 mg per kilogram of body weight. The drug must be taken once daily as a single dose immediately before bedtime. The duration of therapy typically spans from 6 months to 2 years. To prevent recurrent cholelithiasis, administration should continue for 3–4 months after complete stone dissolution has been documented.
- Dose in Biliary Reflux Gastritis: the standard dose is 250 mg (one capsule or tablet) taken once daily before bedtime. The treatment duration generally ranges from 10–14 days up to 6 months.
- Dose in Pediatric Cystic Fibrosis: the recommended starting dose for children aged 6 years and older is 20 mg per kilogram of body weight per day, split into 2–3 doses. If clinically required, the dose may be titrated up to a maximum of 30 mg per kilogram of body weight per day.
- Administration Method: tablets or capsules must be swallowed whole without chewing and washed down with a sufficient volume of water. Strict adherence to the daily dosing schedule is required.
- Missed Dose: if a dose is missed, it should be taken as soon as remembered. If the time for the next scheduled dose is near, the missed dose must be omitted. Taking a double dose to compensate for a missed one is strictly prohibited.

