Azacitidine – Hypomethylating Agent and Antimetabolite Therapy
Known as original brand(s)
Vidaza
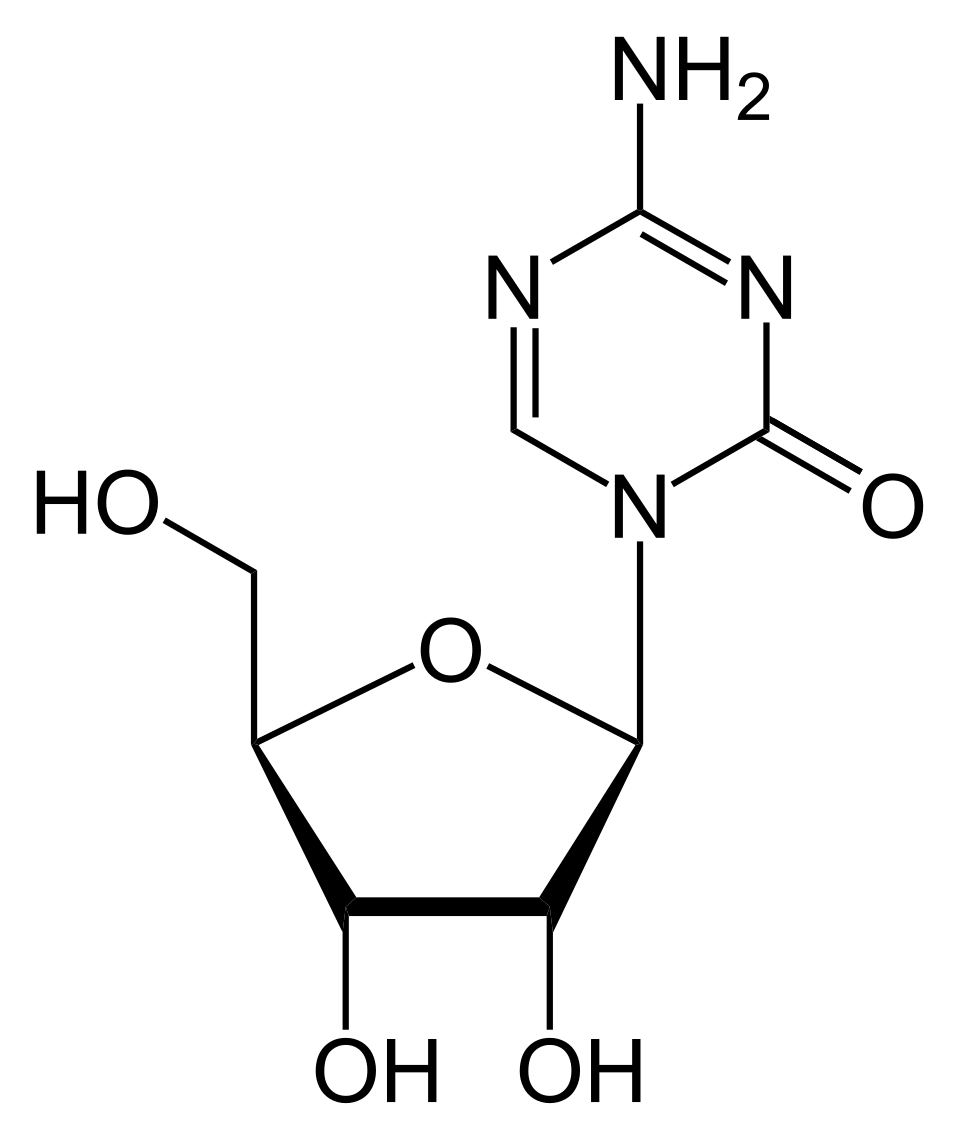
Azacitidine is a cytotoxic antimetabolite functioning as a pyrimidine nucleoside analogue of cytidine. It represents a first-in-class hypomethylating agent engineered for the precision oncology therapy of myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML). The drug delivers a unique, dose-dependent dual mechanism of action aimed at reprogramming the epigenetic landscape of malignant cells. At lower therapeutic concentrations following intracellular transport, azacitidine undergoes phosphorylation and incorporates directly into the DNA architecture, where it covalently binds to and irreversibly inhibits DNA methyltransferase enzymes (specifically DNMT1). This results in profound hypomethylation of previously silenced promoter regions within tumor suppressor genes, restoring normal transcriptional pathways, reactivating cell differentiation cascades, and halting uncontrolled clonal proliferation. At higher concentrations, azacitidine incorporates predominantly into cellular RNA strands, causing critical disruption of RNA processing, profound suppression of protein synthesis, and direct cytotoxic lysis of aberrant cells in the S-phase of the cell cycle.
The clinical uniqueness of azacitidine lies in its documented capacity to significantly prolong overall survival and delay transformation to acute leukemia in high-risk MDS populations compared to standard care regimens. Pharmacokinetically, the drug is rapidly and completely absorbed following subcutaneous administration, reaching peak plasma exposure within 30 minutes. Its absolute bioavailability is approximately 89%. Azacitidine undergoes rapid spontaneous hydrolysis and extensive deamination mediated by cytidine deaminase in the liver and peripheral tissues, converting into inactive metabolites. The plasma elimination half-life is remarkably brief (approximately 40 minutes), and systemic clearance is achieved predominantly via the kidneys in the urine.
The drug is administered subcutaneously or taken orally, depending on the approved formulation. Prior to initiating each subsequent treatment cycle, verification of complete blood counts is mandatory to assess baseline myelosuppression, along with monitoring serum creatinine and hepatic transaminases. Vigilant tracking of hematologic toxicity and structured adjustments to cycle intervals are required throughout therapy.
Indications
Azacitidine is indicated as a systemic targeted chemotherapy for adult patients with the following malignant hematological conditions:
- Myelodysplastic Syndromes (MDS): treatment of adult patients with intermediate-2 and high-risk MDS according to the International Prognostic Scoring System (IPSS), as well as chronic myelomonocytic leukemia (CMML) without leukemic transformation.
- Acute Myeloid Leukemia (AML): systemic treatment of adult patients with newly diagnosed AML harboring 20% to 30% bone marrow blasts and multilineage dysplasia, or as maintenance therapy for patients in first complete remission who are not candidates for hematopoietic stem cell transplantation.
Dosage and administration
The dosing regimen of azacitidine is strictly cyclic, with individual dose calculations based on the patient's body surface area (BSA) and structured step-down adaptations in the event of persistent cytopenias.
- Standard Dose: the recommended starting dose for the initial treatment cycle is 75 mg/m² of the patient's calculated body surface area.
- Schedule and Duration: the drug is administered daily for 7 consecutive days, followed by an obligatory 21-day rest period, completing a standard 28-day cycle. A minimum of 6 cycles is recommended to achieve an optimal clinical response; therapy is maintained as long as clinical benefit is derived.
- Administration Method: for parenteral administration, the reconstituted suspension must be injected subcutaneously into the thigh, abdomen, or upper arm. Sequential injections should be spaced at least 2.5 cm apart from previous sites, completely avoiding areas of erythema, inflammation, or induration. The syringe must be shaken vigorously before handling.
- Missed Dose: if a scheduled dose is missed, it must be administered as soon as possible on the same day. If a same-day catch-up is impossible, the missed dose should not be doubled; instead, the patient resumes the regular schedule the following day, effectively extending the cycle by one day.
- Dose Modification for Toxicity: upon development of severe hematologic toxicities (absolute neutrophil count falling below 1.0 x 10⁹/L or platelets below 50.0 x 10⁹/L), the next cycle must be delayed until peripheral counts recover. Upon resumption, the dose is reduced by 50% or 33% depending on the duration of the cytopenia.